
Detailed Review of the Maskin® Protocol for Meibomian Gland Probing
Meibomian Gland Probing is a straightforward procedure to release periductal fibroses from Meibomian Glands, freeing glands from strictures that block the flow of indispensable meibum.
It is essential to treat comorbid diseases (such as aqueous tear deficiency, allergy, and anterior blepharitis). Without sufficient treatment for root causes of dry eye, patients will experience a reduced duration of sustained benefits and require more frequent probing. On average, annual probing is recommended for maintenance as Meibomian Gland disease progresses in a subclinical manner.
Tips for Patient Care during the Probing Procedure:
Discuss how inhibited flow of meibum results in disease progression.
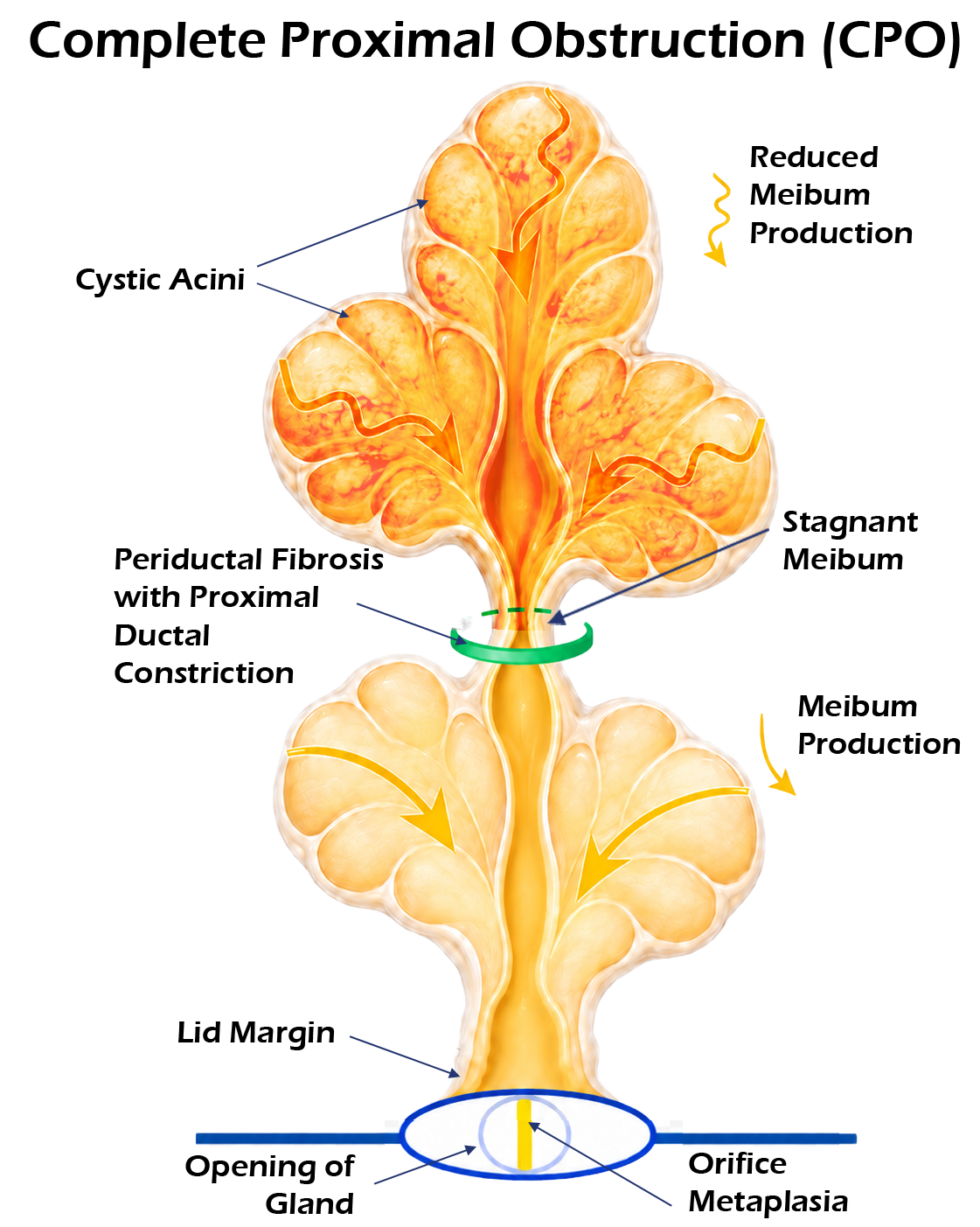
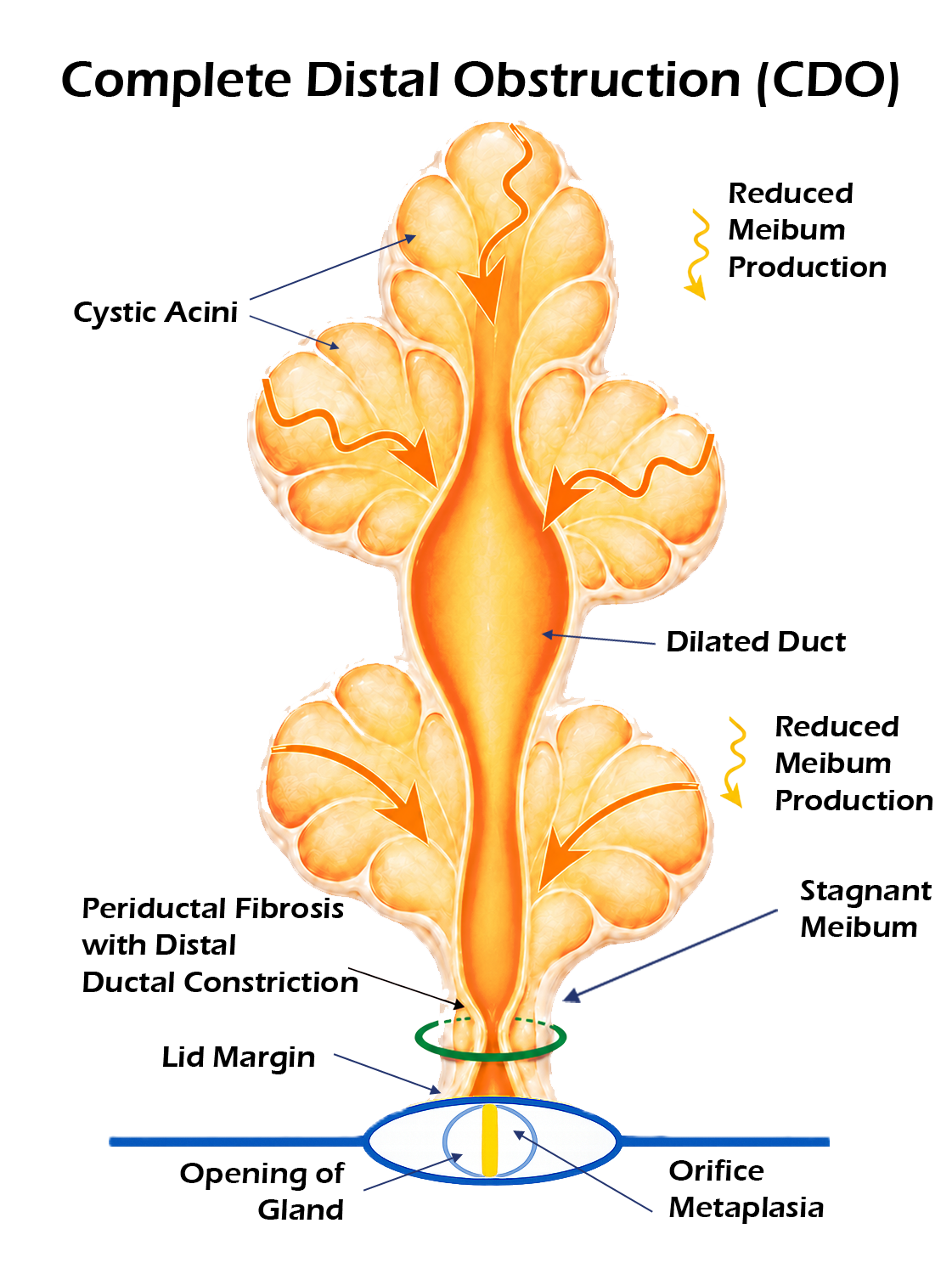
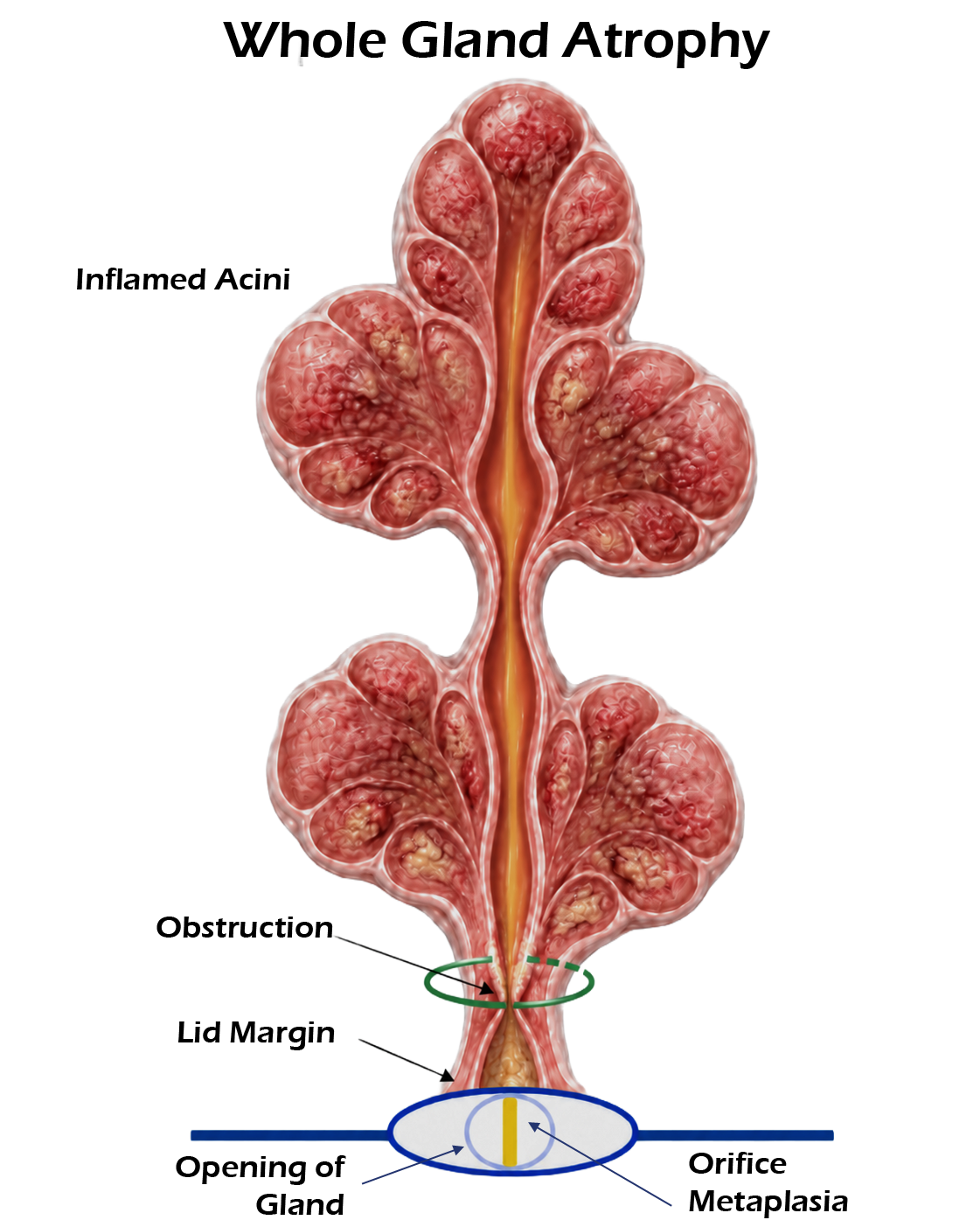
Gland illustrations (available for download) can be used to describe different states of strictures and the risk of progressive gland atrophy.
Review symptoms, such as lid tenderness (LT), burning, and sensitivity to light (photophobia).
Count functional glands both pre-probing and in post-probing follow up visits so the patient is aware of their starting point and progress.
Let the patient know the procedure in its entirety prior to beginning. Share how many glands you expect to probe for each lid.
Consider performing probing of all 4 lids across multiple visits.
Explain sensations the patient may feel throughout the procedure.
Mild burning immediately after jojoba anesthetic ointment is applied to the lids, dissipating in 60 seconds.
Instruct the patient to ask for more anesthetic if feeling pain during the procedure.
The patient may feel or hear subtle pops as each gland is probed, indicative of equilibration of pressure and release of constrictions.
Explain the role of comorbidities in gland health and the recommendation for treatment. Remind patients glands may occlude again if the root cause is not treated adequately.
Prepping for Meibomian Gland Probing (PRIor to START):
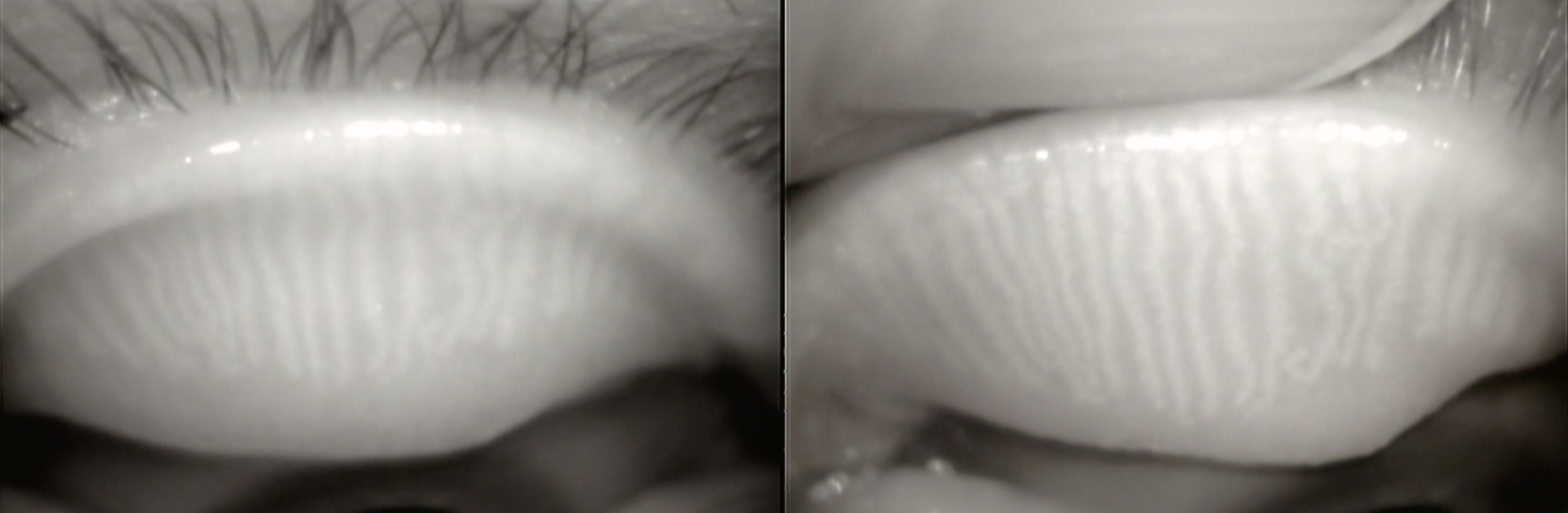
Evaluate patency of orifice, gland proximal and distal atrophy, gland length, and ductal dilation using slit lamp with trans-illumination and/or meibography.
Palpate glands individually to evaluate tenderness and number of expressible glands.
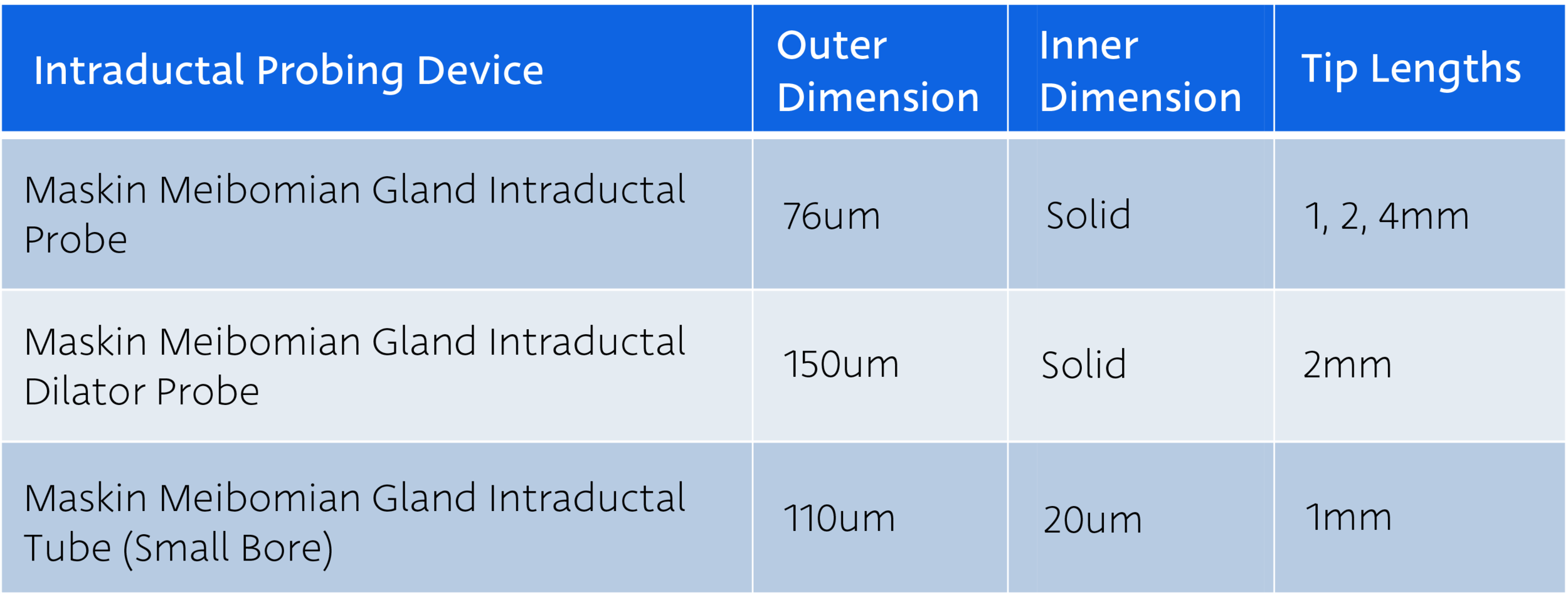
Confirm multiple probes of each length are available for the procedure.
While infrequent, probes may occasionally bend during the probing procedure due to resistance from heavy scarring around glands. If this happens, switch out the probe for a new unit of the same length.
At a minimum, always have the 1mm probe to most efficiently and effectively clear scarring near the gland orifice.
Refrigerate jojoba anesthetic ointment until use. Upon completion of procedure, return to refrigerator. Ointment loses potency within approx. 2 months.
When probing at the slit lamp, a team member can optionally place a hand behind the patient’s head to help keep the patient’s head stable throughout the procedure.
Maskin® Protocol for Meibomian Gland Probing Procedure:



Put 1 drop of proparacaine 0.5% or tetracaine 0.5% solution in the conjunctival sac.
Place bandage contact lens.
Distribute a generous amount of jojoba ophthalmic anesthetic ointment (about the size of a marble) on lower lid margin using sterile cotton-tipped applicator. Application should be abundant enough to visibly coat the lower lid margin with a thick layer of anesthetic. (Use a topical ointment with high percentage of lidocaine or similar).
Have patient close lids for 10 minutes. Burning from ointment dissipates over 60 secs.
If numbing is insufficient for patient comfort, repeat application.
After 10 minutes, place an additional drop of topical anesthetic solution in the conjunctival sac to eliminate possible mild burning when eyes are opened. If comfortable and able, a localized nerve block can be performed for patients with high sensitivity.
Begin probing with the shortest and stiffest probe, the 1 mm length.
Seat probe tip on the orifice then advance through with a dart-like motion.
Adjust location and angle of probe to find proper entry position, especially in cases of cicatricial MGD.
For difficult or occult orifices, use slit lamp red free light or transilluminate lid.
When resistance is encountered, confirm probe is co-linear to the gland then use mild additional force to pop through internal lumen strictures, similar to popping a thin lacrimal punctal scar.
Use longer probes (2mm, 4mm) if persistent LT suggests deeper obstruction.
Expression may be performed using Maskin® Meibum Expressor or other method.
Avoid applying excessive direct pressure on the lid during expression. The glands are sensitive tissues that should not be subjected to trauma.
Inject therapeutic into glands using Maskin® Intraductal Microtube, if indicated. See MG Injection Guide for additional detail.
Remove bandage contact lens.
Rinse eye copiously with sterile preservative-free saline and use cotton-tipped applicator to remove all residual anesthetic from lid margin and lashes.
Give patient preservative-free artificial tears to use every hour until bedtime.